
The Architecture of Hearing | Am I Listening?
The difference between hearing and listening is not a metaphor. It is muscle tone in the middle ear.
Long before you could see, before you could speak, before you had any sense of yourself as a separate being, you could hear.
By the twentieth week of gestation, the cochlea is functional. By the twenty-fourth week, it has reached its mature size, and you have begun to respond consistently to sound. For the remaining four months of life inside another body, you listened to your mother’s voice conducted through bone and fluid, to her heartbeat, the first rhythm you ever knew. You did not choose to hear. Hearing chose you. And it began before anything else.
An architecture you do not notice
A pressure wave moves through air, arrives at the outer ear, and strikes the eardrum, a membrane thinner than a sheet of paper. Behind it, three of the smallest bones in the human body, the malleus, incus, and stapes, form a lever system that amplifies the vibration twenty-two-fold. They have to, because the fluid in the inner ear is so much denser than air that without this amplification, more than 99 percent of the sound energy would simply bounce off.
From there, the vibration enters the cochlea, a spiral the size of a small pea, and ripples a strip of tissue called the basilar membrane. High pitches vibrate one end. Low pitches vibrate the other. Fifteen thousand hair cells translate the motion into electrical signals. Twenty milliseconds later, the auditory cortex has assembled the sound, located it in space, compared it between your two ears, and recognised what it means.
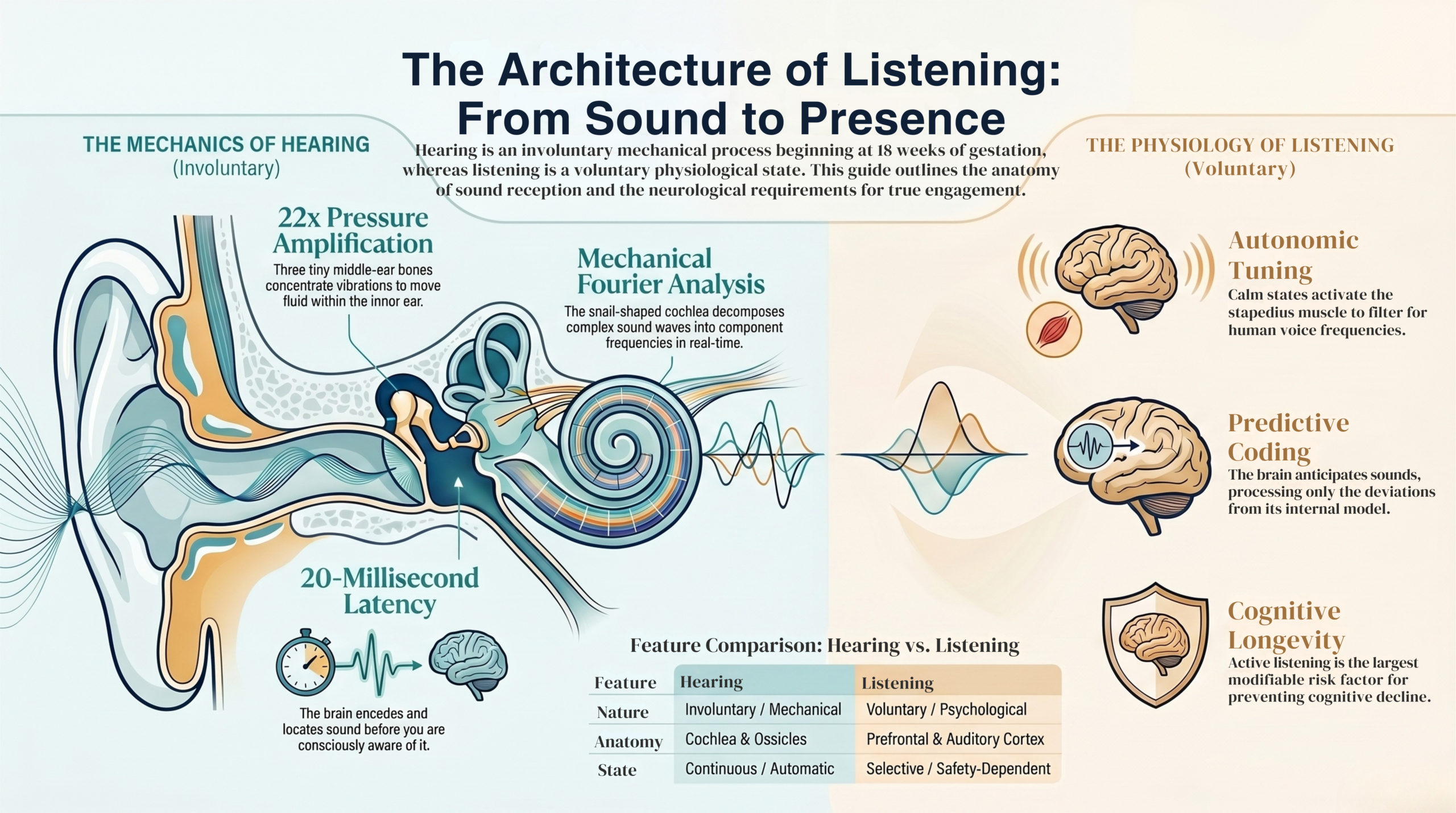
This is the most temporally precise sensory system the human body possesses. And almost none of it asks for your attention.
Hearing is automatic. Listening is not.
The cochlea is perceiving whatever pressure waves arrive at it. The auditory cortex, working with attentional networks in the prefrontal cortex, decides what those signals will become. The two systems are anatomically continuous and operationally distinct, and almost every difficulty in human communication lives in the gap between them.
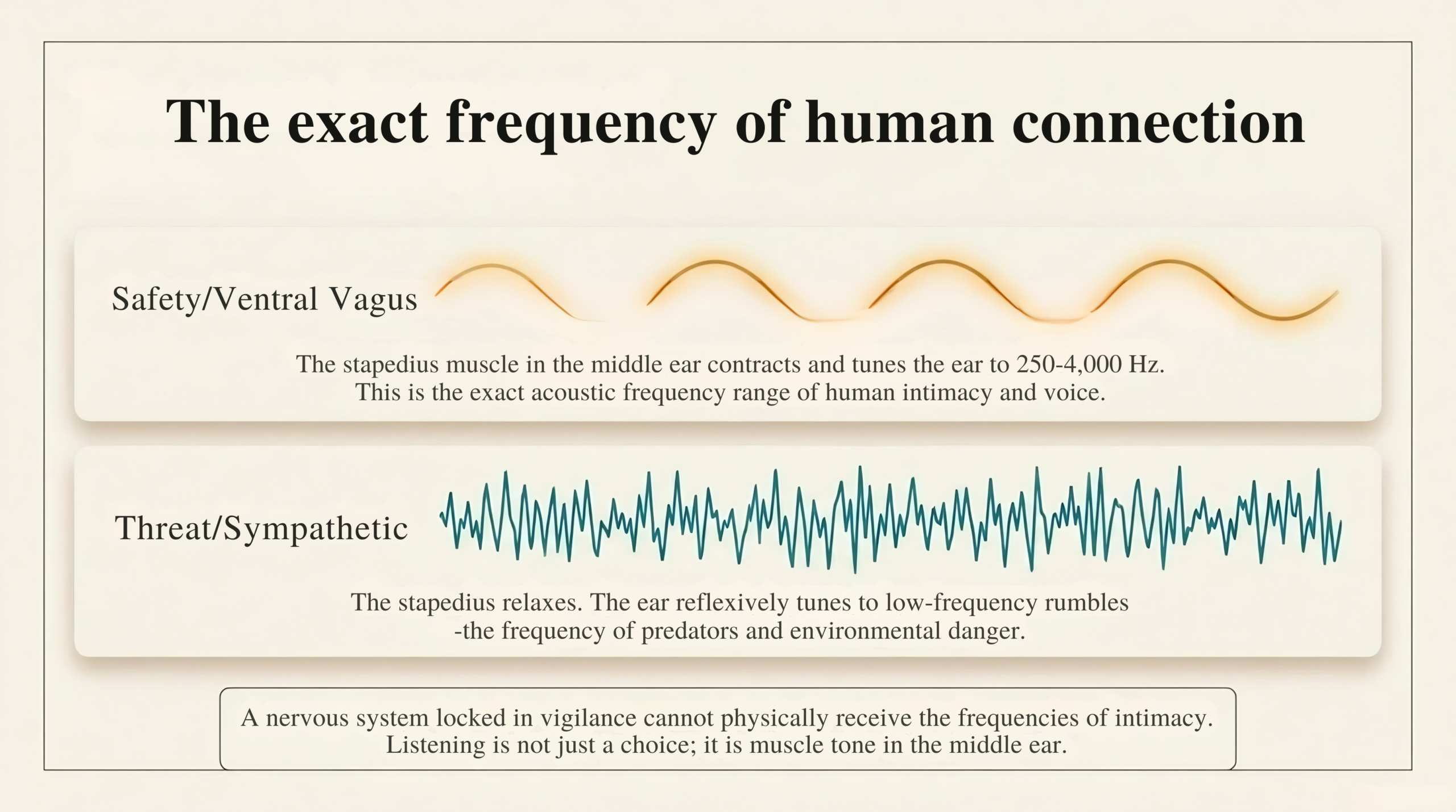
There is one more piece of physiology that changes everything. The middle ear contains a tiny muscle called the stapedius, which adjusts the tension of the ossicular chain. When you are calm, when the ventral branch of your vagus nerve is active, the stapedius tunes the ear toward the frequency range of human voice, roughly 250 to 4,000 Hertz. When your attention shifts towards a threat, the stapedius relaxes, and the ear becomes more sensitive to low frequencies, the rumble of predators, the warning sounds the nervous system has been listening for since long before language.
The key insight
The state of your nervous system shapes what you are capable of hearing. A person locked in chronic stress does not hear human voices the way a calm person does. The frequencies of intimacy are physiologically harder to receive when the body is preparing for danger. This is not a metaphor. It is muscle tone in the middle ear.
Three ways the system breaks
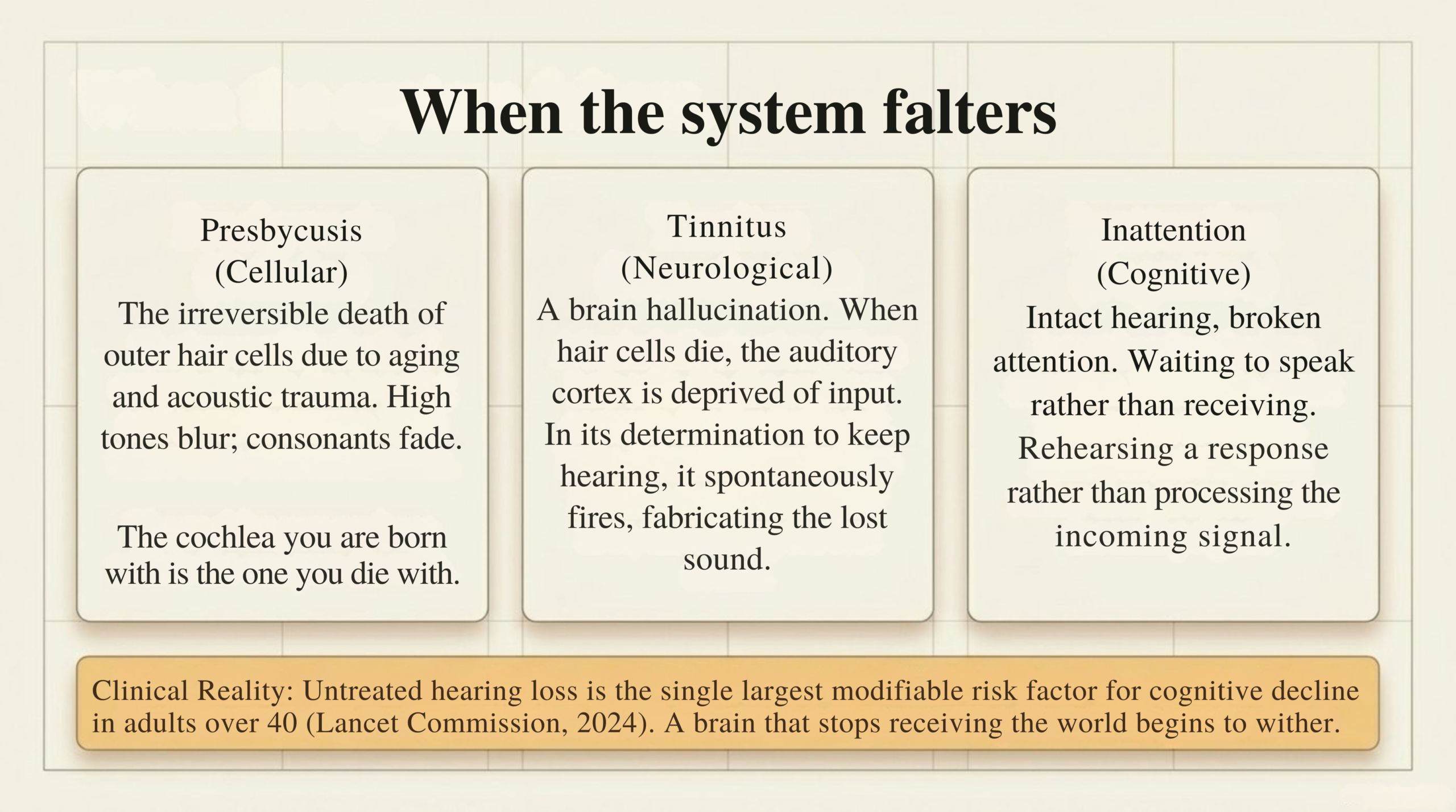
Presbycusis, the gradual loss of hearing that accompanies age, is caused by the death of outer hair cells in the cochlea. Hair cells do not regenerate in humans. The cochlea you were born with is the cochlea you will die with, minus what time and noise have taken away. The World Health Organization estimates that over one billion young people worldwide are at risk of preventable hearing loss from amplified sound through personal audio devices.
Tinnitus, the perception of sound when no external sound is present, affects an estimated fifteen percent of adults. In most cases, it is not an ear problem; it is a brain problem. When hair cells die, the auditory cortex no longer receives input at those frequencies. Deprived of a signal, it begins to fire spontaneously. The brain, in its determination to keep hearing what it has lost, hallucinates.
Inattention, the quietest dysfunction, requires no diagnosis at all. In the consulting room, I see patients whose audiograms are perfect and who have, somewhere along the way, stopped listening. Their hearing is intact. Their attention is not. They wait for me to finish so they can speak again. They have not heard me. They have heard the sound of my voice. The two are not the same.
The Lancet Commission on Dementia Prevention, in its 2024 update, identified untreated hearing loss as a leading modifiable risk factor for dementia from midlife. The mechanism is still studied, but the leading hypothesis is straightforward: a brain that stops receiving sounds will stop engaging with the environment, and a brain that stops engaging the world begins to wither. To stop listening is, eventually, to stop thinking. The cost of inattention is not only relational. It is neurological.
What the ancient traditions already knew
Two great medical systems considered the ear with a seriousness that Western medicine has only recently recovered. Ayurveda associated the ear with the element of space and prescribed warm medicated oil in the ear canal — karṇa pūraṇa — for tinnitus, vertigo, and restlessness. The auricular branch of the vagus nerve runs through the ear canal. Warm oil there is, neurologically, vagal stimulation, something that modern medicine now calls transcutaneous auricular vagus nerve stimulation, currently being studied for anxiety, depression, and tinnitus.
Traditional Chinese Medicine associated the ear with the kidneys, by foundational vitality. Anatomically improbable, until you remember that the cochlea is among the most metabolically demanding tissues in the body, sustained by an ionic gradient that depends on systemic metabolic health. Chronic kidney disease does produce measurable hearing loss. The traditional physician was observing a real association in the only vocabulary available.
Modern neuroscience has added something both traditions sensed but could not measure: the brain does not passively receive sound. It actively predicts it. The auditory cortex generates an internal model of what it expects to hear next, and processes the discrepancy between expectation and arrival. This is why your name across a crowded room reaches you instantly. It is also why the person who habitually finishes other people’s sentences in their head has stopped listening; they are hearing their own model of the conversation, not the conversation itself.
The ear is the closest doorway the nervous system has to itself.
Are you listening?
The question is not whether the cochlea is working. The cochlea has been hearing since you were twenty weeks old, and it has not paused. The question is whether we practice the voluntary, attentive, autonomically settled, prediction-suspended act we call listening. For most people, on most days, the honest answer is no.
You are listening when the predictions stop. When the cortex is no longer racing ahead of the conversation, finishing the sentence before it has been spoken. When the body has settled enough so that the middle ear is tuned toward the human voice rather than a threat. When attention is in the room with the sound, rather than in the next moment with the response.
A patient I saw years ago articulated this idea more precisely than I ever could. She had been suffering from a vestibulo-cochlear condition. The diagnosis turned out to be straightforward, and the treatment simple. But what she said at the end of the consultation has stayed with me: I think I stopped hearing people years ago. I was so busy preparing my response to the bad news that I couldn’t be in any conversation that wasn’t about it. She had not lost her hearing. She had lost the silence around the sound. And the silence around the sound is where listening lives.
The ear is built for this. It is waiting, the way it has been waiting since you were twenty weeks old, for you to stop performing and start listening.
Free Download
The Still Listen
A printable 5-minute daily practice card — to use in the first minutes of waking, before a difficult conversation, or at the close of the day.
Read further
This piece is a summarized web version from the corresponding chapter of Anatomy of Being, a book about the body as a system of meaning. The full chapter explores contemplative traditions, the eighth-century Kashmiri text on the silence inside every sound, and the practices for returning to listening. Link to the book →
References
Selected sources
- Pickles JO. An Introduction to the Physiology of Hearing. 5th ed. Brill, 2024.
- Friston K. The free-energy principle: a unified brain theory? Nat Rev Neurosci. 2010.
- Porges SW. The Polyvagal Theory. Norton, 2011.
- Livingston G, Huntley J, Liu KY, et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet. 2024; 404: 572–628.
- Hepper PG, Shahidullah BS. Development of fetal hearing. Arch Dis Child. 1994.
- Oliveros P. Deep Listening: A Composer’s Sound Practice. iUniverse, 2005.
A clinical note. This piece is reflective and educational. If you are experiencing new or worsening hearing loss, tinnitus, vertigo, or sudden hearing change, please see an ENT specialist or your GP. Sudden sensorineural hearing loss is a medical emergency; see a doctor the same day.





