By Dr. Carmen Chiran, ENT Specialist · May 2026 · 8 min read
Free Download: The 5 Signs Your Allergies Need an ENT
A printable eight-page guide designed to bring to your GP or specialist appointment. Includes the updated treatment ladder and red flag checklist.
Every spring, the same ritual. Same antihistamine, same struggle, and if you are honest with yourself, symptoms that feel a little worse than last year. If that sounds familiar, I want to tell you something important: you are not imagining it.
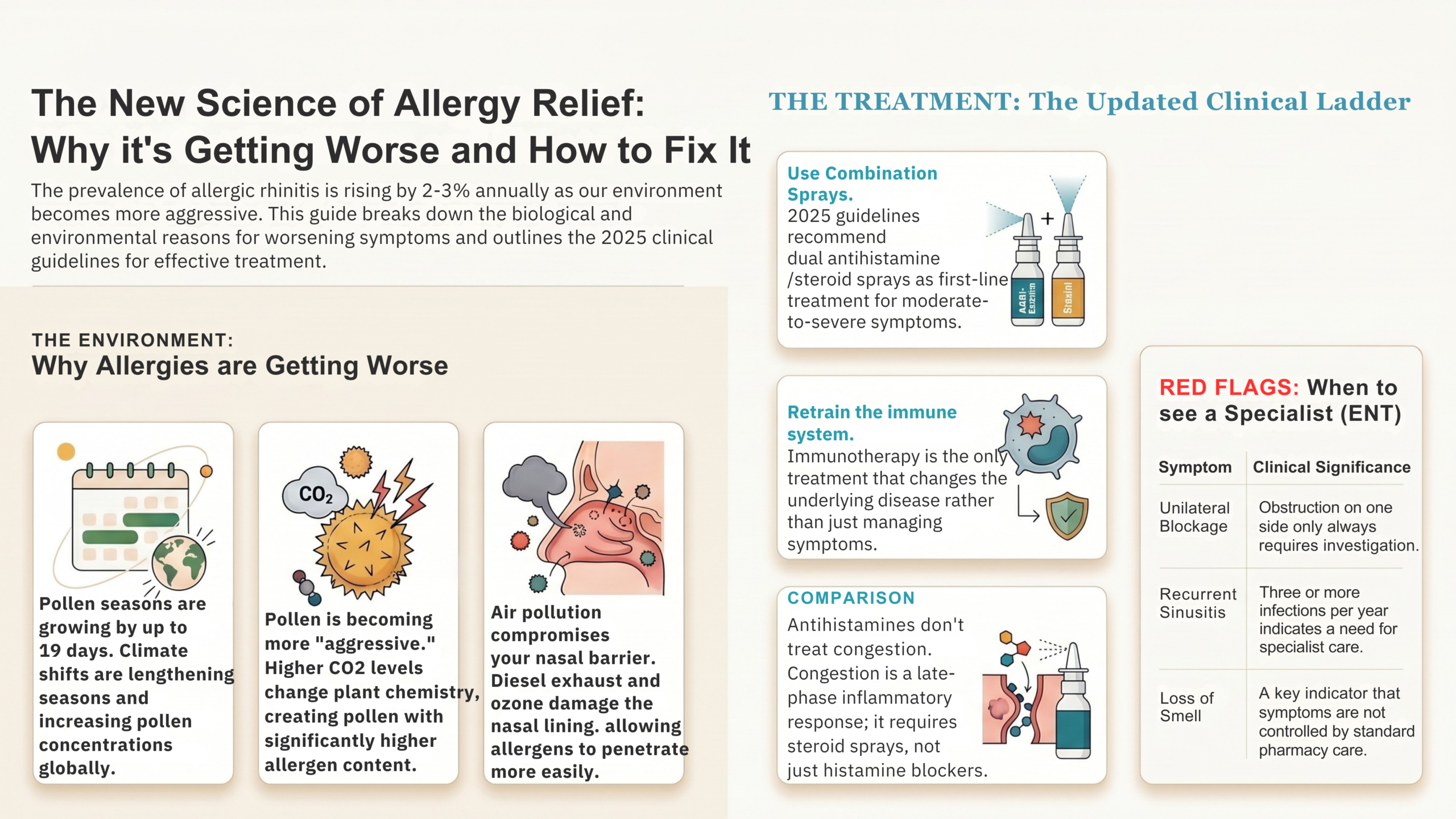
Allergic rhinitis prevalence has increased by two to three percent every single year for the past two decades. Pollen seasons are already measurably lengthening in many regions, with studies projecting they could grow by up to 19 additional days. And the clinical guidelines for treating this condition were significantly updated in 2024–2025, in ways that most patients and many doctors have not yet heard about.
In this article, I am going to explain three things: why your allergies are genuinely getting worse, why the most common treatment misses your worst symptom, and what the current evidence actually recommends. By the end, you will have a framework, not just a list of tips.
The new science of allergy relief: why it is getting worse, and what the updated guidelines now recommend.
What Is Allergic Rhinitis? The Mechanism Most Patients Were Never Told
Most people with allergic rhinitis have had it explained to them in about thirty seconds. You are allergic to pollen. Take an antihistamine. Avoid being outside on high-pollen days. That explanation is not wrong, but it leaves out almost everything that would actually help you.
Here is the real version. Your immune system keeps a filing system. Everything it encounters gets assessed as harmless or a threat. Most things are filed under harmless and forgotten. But some things get flagged, placed in a special folder, and marked for immediate response every time they appear.
In people with allergic rhinitis, pollen ends up in that folder. Not because pollen is dangerous (it is not), but because somehow the immune system made a mistake. It produced antibodies called IgE, specifically designed to recognise that pollen. Those IgE antibodies coat the mast cells lining the inside of the nose.
Your nose is essentially lined with tripwires. On first exposure to pollen, the immune system takes notes, an action called sensitisation, and nothing dramatic happens. During each subsequent exposure, pollen locks on those IgE-coated mast cells. They start releasing histamine, leukotrienes, and prostaglandins in a cascade that produces your symptoms.
This cascade has two phases, and understanding both is essential for correcting the treatment.
The Early Phase (within minutes)
This is the histamine-driven response. Sneezing, itching, watery eyes, and a runny nose. Fast onset, typically resolves within an hour or two. Antihistamines work well here.
The Late Phase (4–6 hours later)
This is where nasal congestion happens. Driven by leukotriene-mediated inflammation and vascular engorgement of the nasal mucosa, it is slower, heavier, and far more disabling for most chronic sufferers. And this is where antihistamines largely fail, because histamine is barely involved.
We will come back to this in a moment. First, the bigger picture.
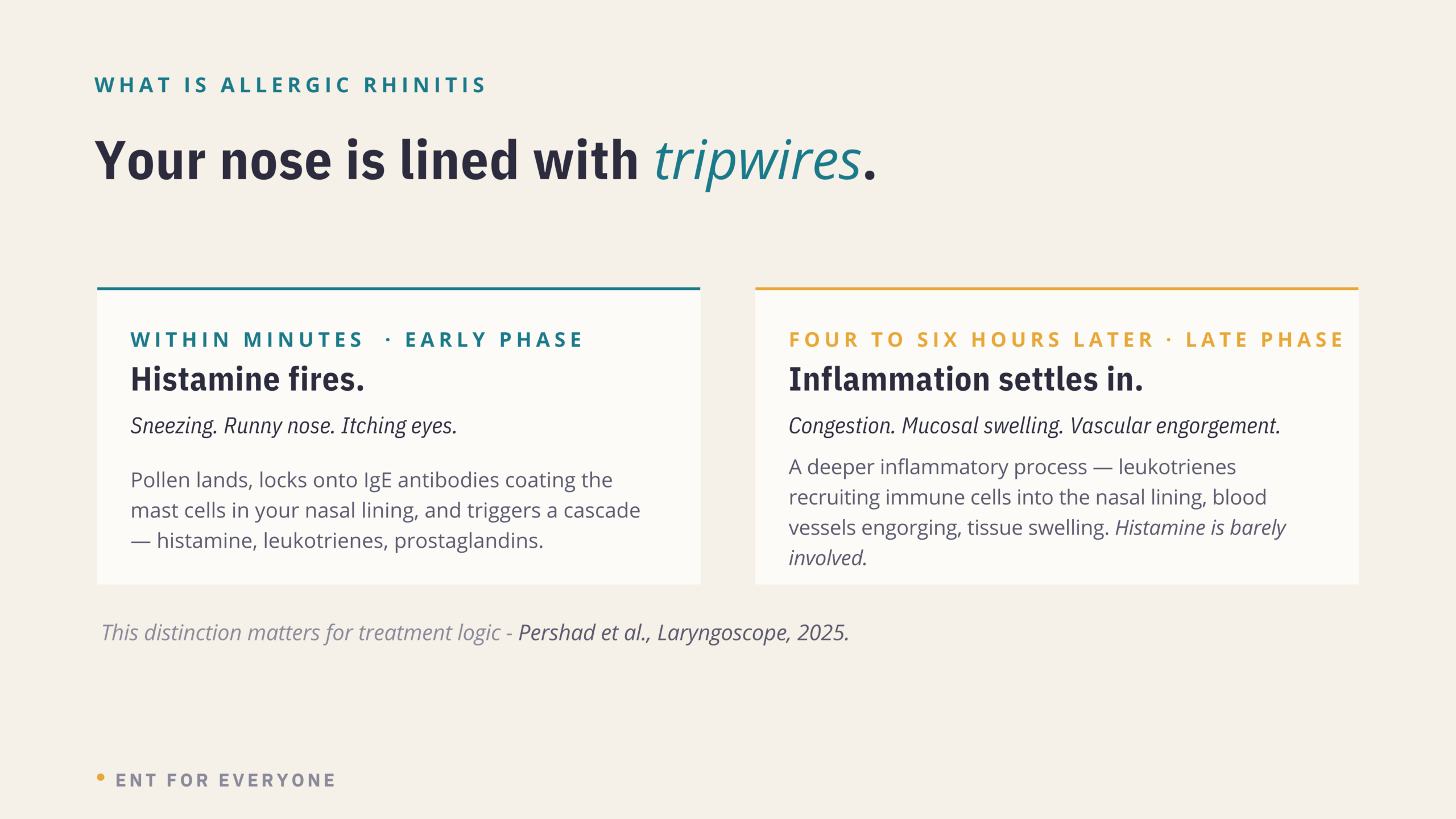
The two-phase allergic response. The early phase responds to antihistamines. The late phase, which drives congestion, largely does not.
Why Are Allergies Getting Worse Every Year? Three Documented Reasons
This is not about individual sensitivity increasing over time, though that can happen. The worsening most people notice is driven by three measurable environmental changes.
1. Pollen seasons are lengthening
A 2025 scoping review published in The Laryngoscope, one of the leading otolaryngology journals, analysed thirty studies on climate change and allergic rhinitis. Sixteen reported longer pollen seasons and higher pollen concentrations linked to climate change, with projections estimating pollen seasons could lengthen by up to 19 days and total pollen emissions could increase by up to 40% in North America.1 In many regions, this shift is already measurable rather than merely projected.
2. The pollen itself is more allergenic
Higher carbon dioxide levels do not just make plants produce more pollen. They change the chemistry of the pollen. Plants growing in elevated CO₂ environments produce pollen with higher allergen content. The same quantity of pollen now triggers a stronger immune response than it would have thirty years ago.
3. Your nasal barrier is more vulnerable
Air pollution, specifically diesel exhaust particles and ground-level ozone, directly damages the epithelial barrier lining the nasal passages. Think of that lining as a security system at the front door. Pollution compromises the locks. Pollen that might previously have been caught in the outer nasal passages now penetrates more easily, triggers a stronger response, and takes longer to resolve.
Same person. Same genetics. Different environment. The biology responds to measurable change.

Three reasons. All documented. All measurable.
Why Your Antihistamine Is Not Enough (And What Actually Is)
This is the section I would like you to read carefully because this is where most of the frustration and clinical mismanagement happens.
Antihistamines work. They do exactly what they are designed to do. They block histamine. They reduce sneezing, itching, watery eyes, and runny nose. For mild intermittent symptoms, a second-generation oral antihistamine (cetirizine, loratadine, fexofenadine) remains entirely appropriate first-line treatment.
The problem is nasal congestion.
Congestion, the blocked nose that makes you breathe through your mouth all night, the one that leaves you exhausted and unable to concentrate, is primarily driven by that late-phase inflammatory response. Leukotrienes, mucosal swelling, vascular engorgement. Histamine plays a minor role. An antihistamine does not meaningfully reach this process.
Do not confuse steroid nasal sprays (fluticasone, mometasone, budesonide) with decongestant nasal sprays (xylometazoline, oxymetazoline). Decongestant sprays give fast relief but should never be used for more than three days. Beyond that, they cause rebound congestion — rhinitis medicamentosa — that is often significantly worse than the original symptom. Steroid sprays are safe for long-term daily use.
Intranasal corticosteroid sprays suppress the entire inflammatory cascade, not just histamine, but the full response, including the late phase that drives congestion. They are significantly more effective for nasal blockage than oral antihistamines. They require daily use (not as-needed), take three to five days to reach full effect, and need correct technique: angled away from the septum, not directed straight back.
If you have been taking an antihistamine every day and your nose is still blocked, the antihistamine has not failed you. You were given the wrong tool for that particular symptom.
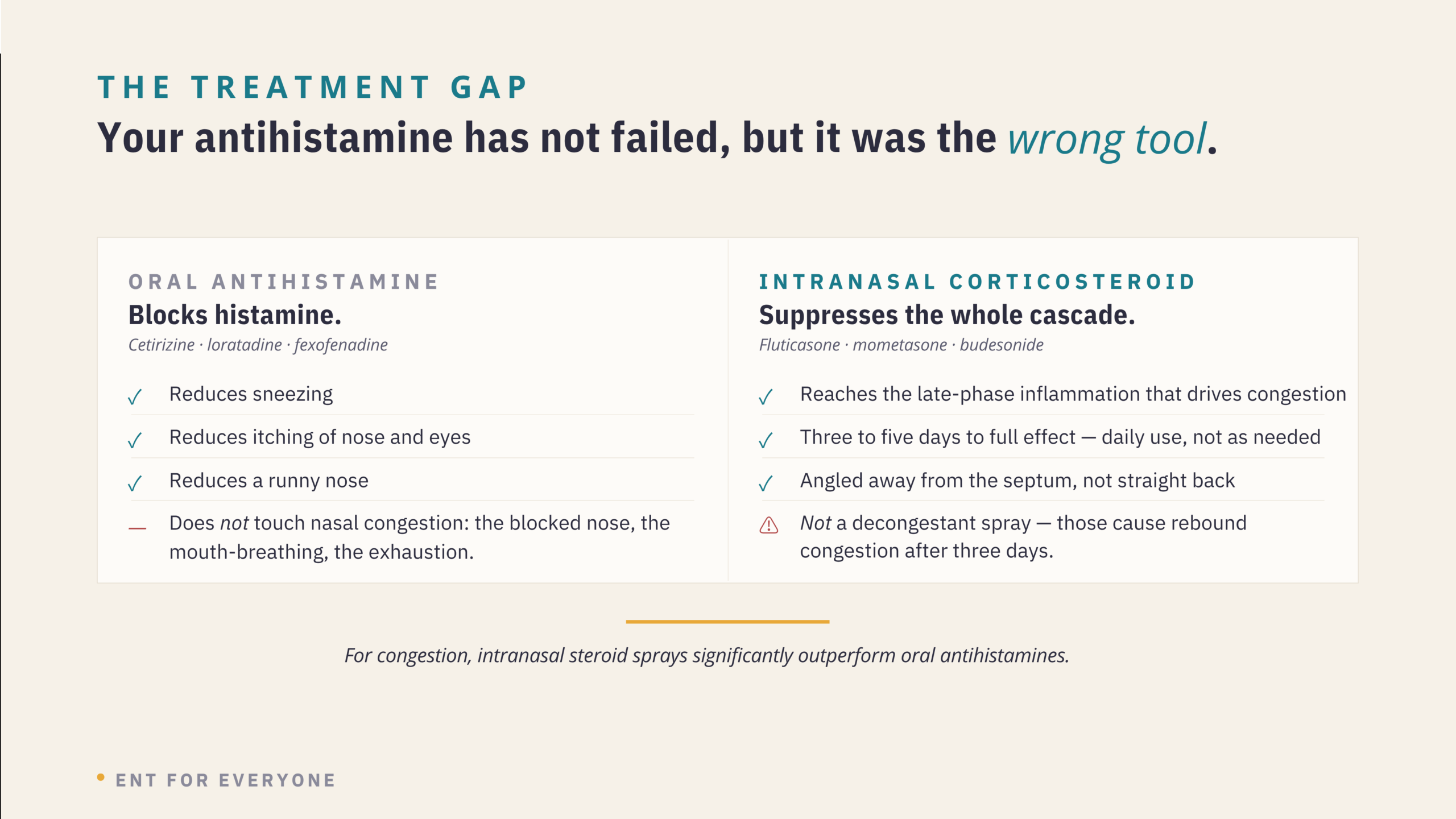
Your antihistamine has not failed. But for nasal congestion, it was the wrong tool. Intranasal corticosteroid sprays suppress the full inflammatory cascade — including the late phase that drives blockage.
The Updated Treatment Ladder: What the 2024–2025 Guidelines Recommend
The Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines, updated in collaboration with the European Academy of Allergy and Clinical Immunology (EAACI) in 2024–2025, represent the international evidence-based standard for allergic rhinitis management.2 Most patients are not aware these guidelines exist, let alone that they were recently updated.
Oral antihistamine — as needed
Second-generation (cetirizine, loratadine, fexofenadine). Non-sedating. For mild, intermittent symptoms. Start before your pollen season begins, not after symptoms are already severe.
Add intranasal corticosteroid spray — daily
Fluticasone, mometasone, or budesonide. Must be used every day, not as needed. Takes 3–5 days to reach full effect. This single addition makes a significant difference for most patients with moderate or persistent symptoms.
Combination spray (intranasal antihistamine + corticosteroid) 2024–25 Update
The 2024–2025 ARIA-EAACI guidelines now recommend a fixed-combination spray — intranasal antihistamine plus intranasal corticosteroid in a single formulation — as first-line treatment for moderate-to-severe symptoms. This is a meaningful change from previous guidance. If you are at this step and this has not been discussed with you, ask about it.
Allergen immunotherapy is the only disease-modifying treatment
Steps 1–3 manage symptoms. Only immunotherapy changes the underlying disease. Subcutaneous injections or sublingual tablets/drops, given in gradually increasing doses over months to years, retrain the immune system’s response to the specific allergen. Requires allergy testing and specialist involvement. Evidence shows meaningful reductions in medication use, reduced risk of developing asthma, and benefits that persist for years after stopping. If you have had moderate-to-severe allergic rhinitis for more than two years and immunotherapy has not been mentioned, it is worth asking.
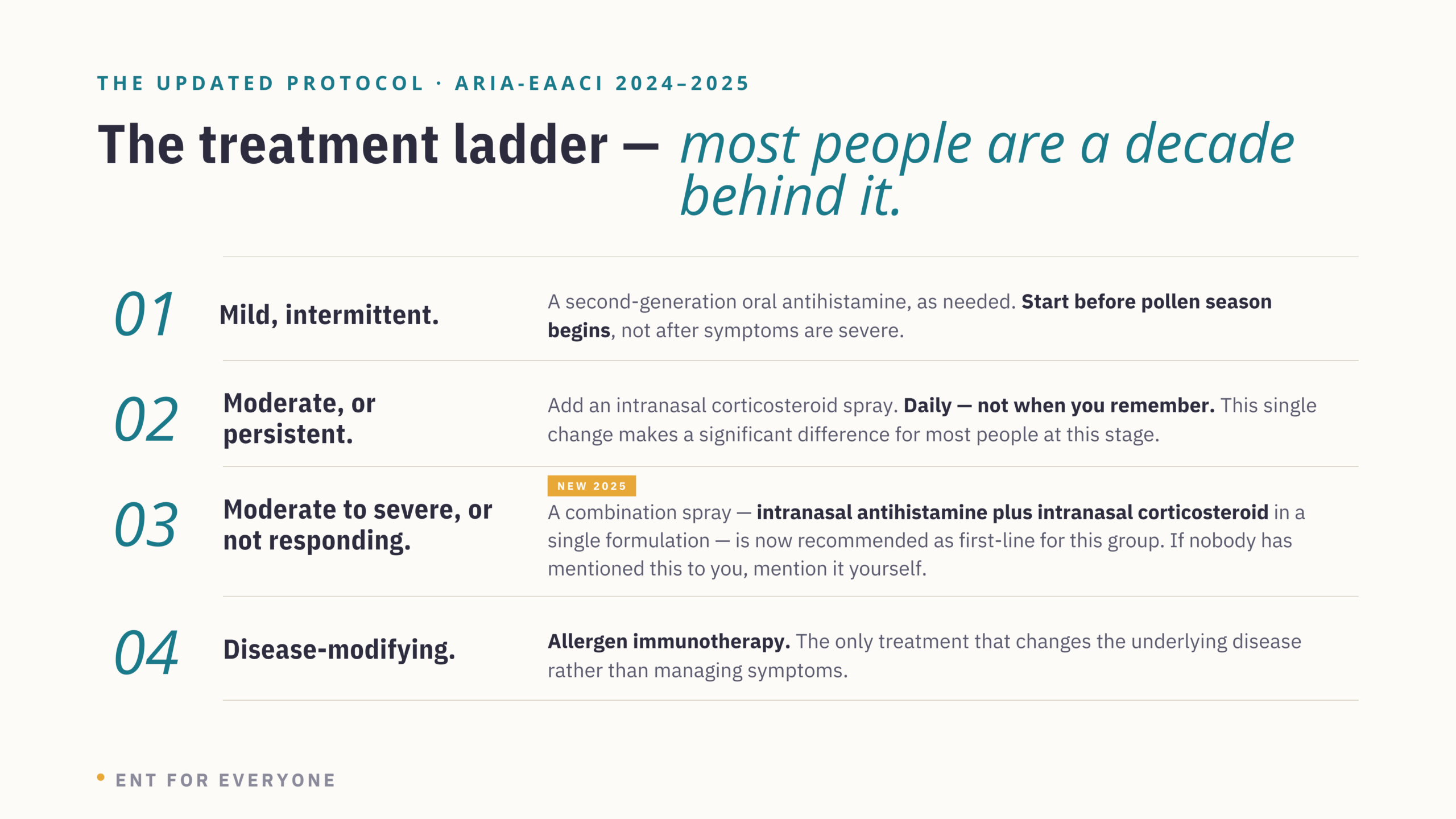
The updated treatment ladder. Most people are still on step 1. Steps 2, 3, and especially 4 are where the evidence now points.
📋 Free: Seasonal Allergy Action Plan
A printable eight-page tracker covering your symptoms, triggers, current treatment step, red flags, and questions to bring to your next appointment.
When to See an ENT Doctor, Not Just a Pharmacy
Your GP is the appropriate first point of contact for most allergic rhinitis. An ENT becomes relevant in the following situations:
| # | Red Flag | Action |
|---|---|---|
| 1 | Symptoms not controlled despite steps 1–3 used consistently and correctly | ENT referral |
| 2 | Nasal obstruction on one side only — unilateral blockage always requires investigation | ENT referral |
| 3 | Loss of smell (anosmia or hyposmia) | ENT referral |
| 4 | Recurrent sinusitis — three or more episodes per year | ENT referral |
| 5 | Considering allergen immunotherapy — requires allergy testing and specialist prescription | ENT or allergist |
Frequently Asked Questions
Why do allergies get worse as you get older?
Two things happen simultaneously. Pollen seasons are lengthening, and pollen allergenicity is increasing, so the external trigger is genuinely stronger year on year. At the same time, cumulative sensitisation means repeated exposures can lower the threshold at which the immune system fires. Neither is inevitable, but together they explain why many people notice a gradual worsening even when their habits have not changed.
Why doesn’t my antihistamine help with a blocked nose?
Nasal congestion is driven primarily by the late-phase inflammatory response — leukotriene-mediated swelling and vascular engorgement — which occurs 4–6 hours after allergen exposure. Antihistamines block histamine, which drives sneezing, itching, and rhinorrhoea but plays a minor role in congestion. Intranasal corticosteroid sprays suppress the full inflammatory cascade and are significantly more effective for nasal blockage.
What is the difference between an antihistamine nasal spray and a steroid nasal spray?
These are different medication classes. Intranasal antihistamine sprays (e.g. azelastine) block histamine locally and act quickly but primarily target sneezing and runny nose. Intranasal corticosteroid sprays (e.g. fluticasone, mometasone) suppress the entire inflammatory response, including congestion, and require daily use for full effect. The updated 2024–2025 ARIA-EAACI guidelines now recommend a combination product containing both as a first-line treatment for moderate-to-severe allergic rhinitis.
What is allergen immunotherapy, and is it available on the NHS?
Immunotherapy is the only treatment that modifies the underlying allergic disease rather than managing symptoms. It involves gradually introducing increasing doses of your specific allergen — as injections or sublingual tablets/drops — to retrain the immune system. Sublingual immunotherapy for grass pollen allergy is available on the NHS in some areas; availability varies. A referral to an NHS allergy clinic or ENT department is the starting point. Private immunotherapy is more widely accessible.
When should I see an ENT for allergies rather than my GP?
Your GP is the right first point of contact. See an ENT if symptoms remain uncontrolled despite optimised pharmacotherapy, if you have nasal blockage on one side only, loss of smell, recurrent sinusitis (3+ episodes per year), or if you want to explore immunotherapy. Structural factors like nasal polyps, deviated septum sometimes underlie treatment-resistant allergic rhinitis and require specialist assessment.
References
- Pershad AR, Krishnan R, Lee E, et al. How climate change is impacting allergic rhinitis: a scoping review. Laryngoscope. 2025;135(8):2670–2682. doi:10.1002/lary.32124
- Sousa-Pinto B, Bousquet J, Vieira RJ, et al. Allergic rhinitis and its impact on asthma (ARIA)–EAACI guidelines — 2024–2025 revision: Part I — guidelines on intranasal treatments. Allergy. 2026;81:663–683. doi:10.1111/all.70159
- Augustin J, Gilge S, Appel H, et al. Climate change, air quality, and pollen allergies — state of the art and recommendations for research and public health. Allergy. 2026;81:663–683. doi:10.1111/all.70159