
In December 2024, something unprecedented in the history of medicine happened: the FDA approved a prescription medication specifically for obstructive sleep apnea.
Not a device. Not a surgery. A weekly injection of the same family of drugs as Ozempic and Wegovy.
The headlines were predictably enthusiastic. Sleep apnea drug approved. Finally, an alternative to the CPAP machine. Could this replace the mask?
Some of that enthusiasm is warranted. This is genuinely significant news, and I want to give it the credit it deserves. But the full picture is more complicated, and if you or someone you love has sleep apnea, you need to understand what this drug actually does, who it helps, and what the coverage is quietly leaving out.
The First Medicine for Sleep Apnea
The drug is called tirzepatide, sold under the brand name Zepbound. It belongs to a class of medications called GLP-1 receptor agonists, the same class as semaglutide (Ozempic, Wegovy) and liraglutide (Saxenda). These drugs work by mimicking hormones that regulate appetite and blood sugar, leading to significant, sustained weight loss.
Zepbound was already approved for obesity. In December 2024, the FDA extended that approval to include moderate-to-severe obstructive sleep apnea in adults with obesity, making it the first pharmacological treatment ever approved for this condition.
That milestone matters. Roughly one billion people worldwide have obstructive sleep apnea. Until now, treatment options were mechanical (CPAP machines, mandibular advancement devices) or surgical. The idea that a medication could meaningfully reduce the severity of sleep apnea opens a genuinely new door. But it only opens that door for a specific group of people, and the drug comes with real limitations that deserve an honest conversation.
The Numbers Are Impressive, But Read Them Carefully
The evidence comes from a large phase 3 trial called SURMOUNT-OSA, published in the New England Journal of Medicine in June 2024. The trial enrolled adults with moderate-to-severe sleep apnea (defined as 15 or more breathing pauses per hour of sleep) and obesity.
At 52 weeks, participants taking tirzepatide experienced a 51–59% reduction in apnea events per hour, compared to around 5% with placebo. Roughly half achieved what researchers called disease resolution. Those are meaningful numbers, and I don’t want to minimize them.
But here is the comparison that matters most clinically: CPAP, when worn consistently, reduces apnea to near-zero in the vast majority of users, eliminating 80–90% of breathing events. Tirzepatide got only about one in three patients to that same threshold. This is not an argument against the drug. It’s context. A 55% reduction in apnea is real and valuable, especially for someone who cannot tolerate wearing a mask every night. But it is not the same as resolving the problem.
How and Why It Works
To understand who this drug helps, you need to understand why it reduces apnea.
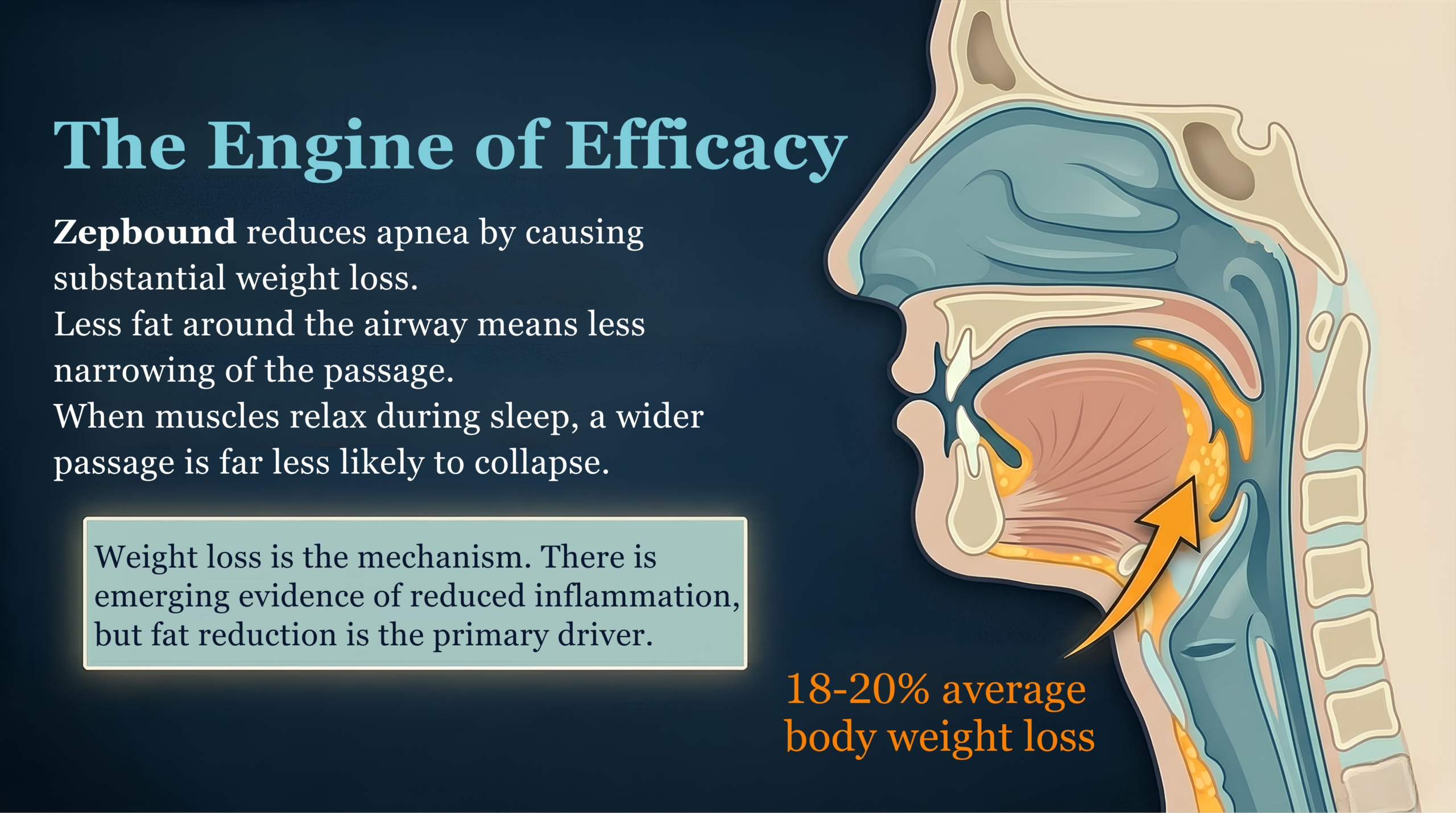
In most people with obstructive sleep apnea, excess weight is the primary driver. Fat deposits around the throat, tongue, and soft palate narrow the upper airway. When the muscles relax during sleep, that narrowed passage collapses and breathing pauses. Zepbound causes substantial weight loss, averaging 18–20% of body weight in the trial. Less fat around the airway means less collapse. It is, at its core, a very effective way to achieve what we’ve always known would help: significant, sustained weight reduction.
There is emerging evidence that the drug may also have some direct effects on airway inflammation and nerve signaling in the throat, but these appear to be secondary. Weight loss is the engine here.
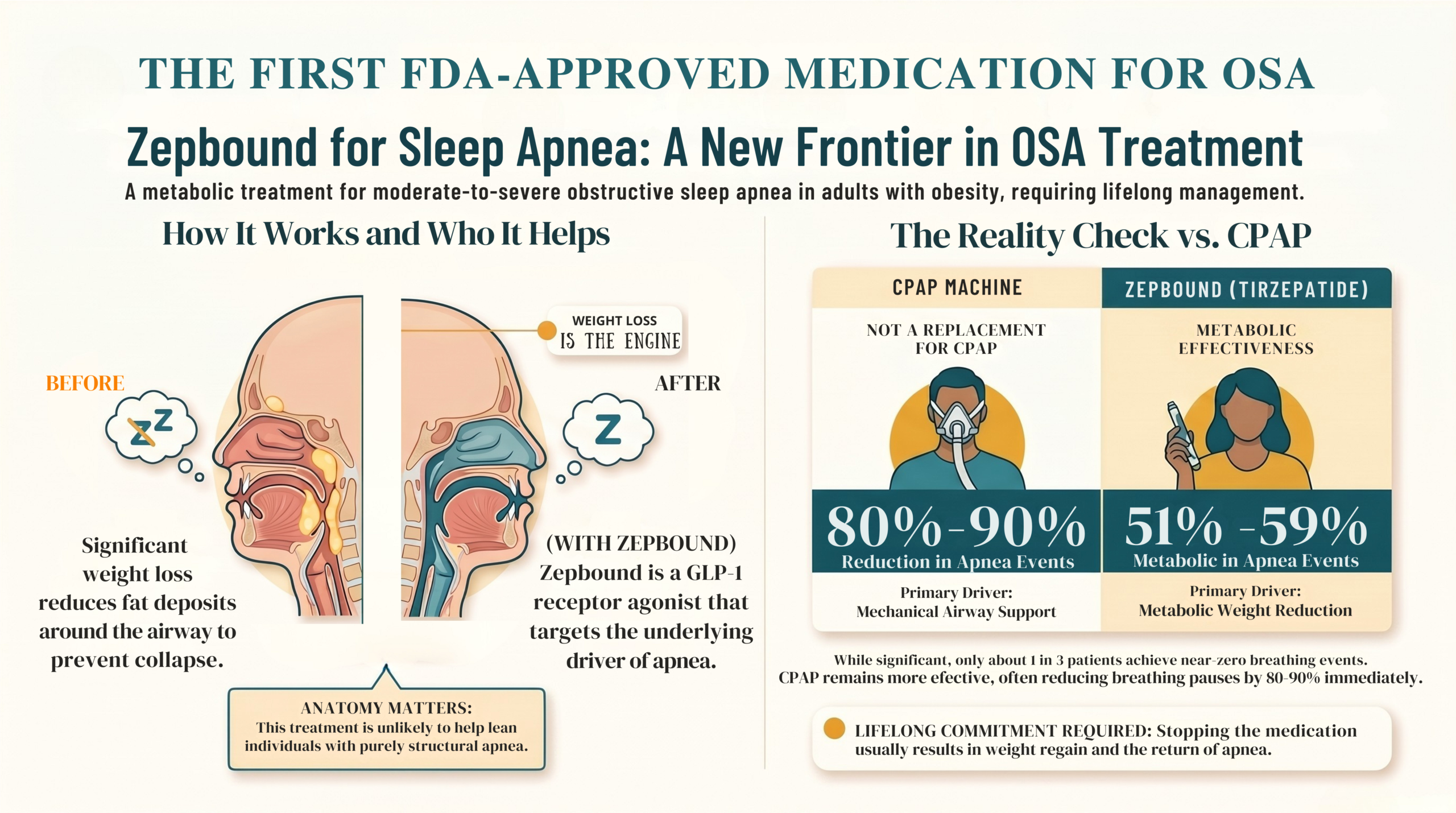
This has one very important implication: if obesity is not the primary cause of your sleep apnea, this drug is unlikely to help you.
Sleep apnea in lean individuals is usually driven by specific anatomical factors: the shape of the jaw, the position of the tongue, the size of the tonsils, or the structure of the nasal airway. No amount of weight loss addresses a jaw that sits too far back. That is a different problem requiring a different solution.
The Two Risks That Are Not Getting Enough Attention
This is the part of the story that the enthusiastic headlines tend to skip.
When You Stop, the Weight Comes Back and So Does the Apnea
GLP-1 medications do not cure obesity. They manage it in the same way that blood pressure medication manages hypertension. Stop the drug, and the biology that drives the weight gain resumes.
Studies show that more than half of people who discontinue GLP-1 therapy regain most of their lost weight within a year. The airway fat returns. The apnea returns with it.
This means Zepbound is not a course of treatment with an endpoint. For the benefits to persist, the medication must continue, potentially for life. That has significant implications for cost, access, and long-term planning, all worth thinking through carefully before starting.
You Are Not Just Losing Fat
This is the risk I find most underappreciated in current coverage, and one I want to be direct about as a clinician.
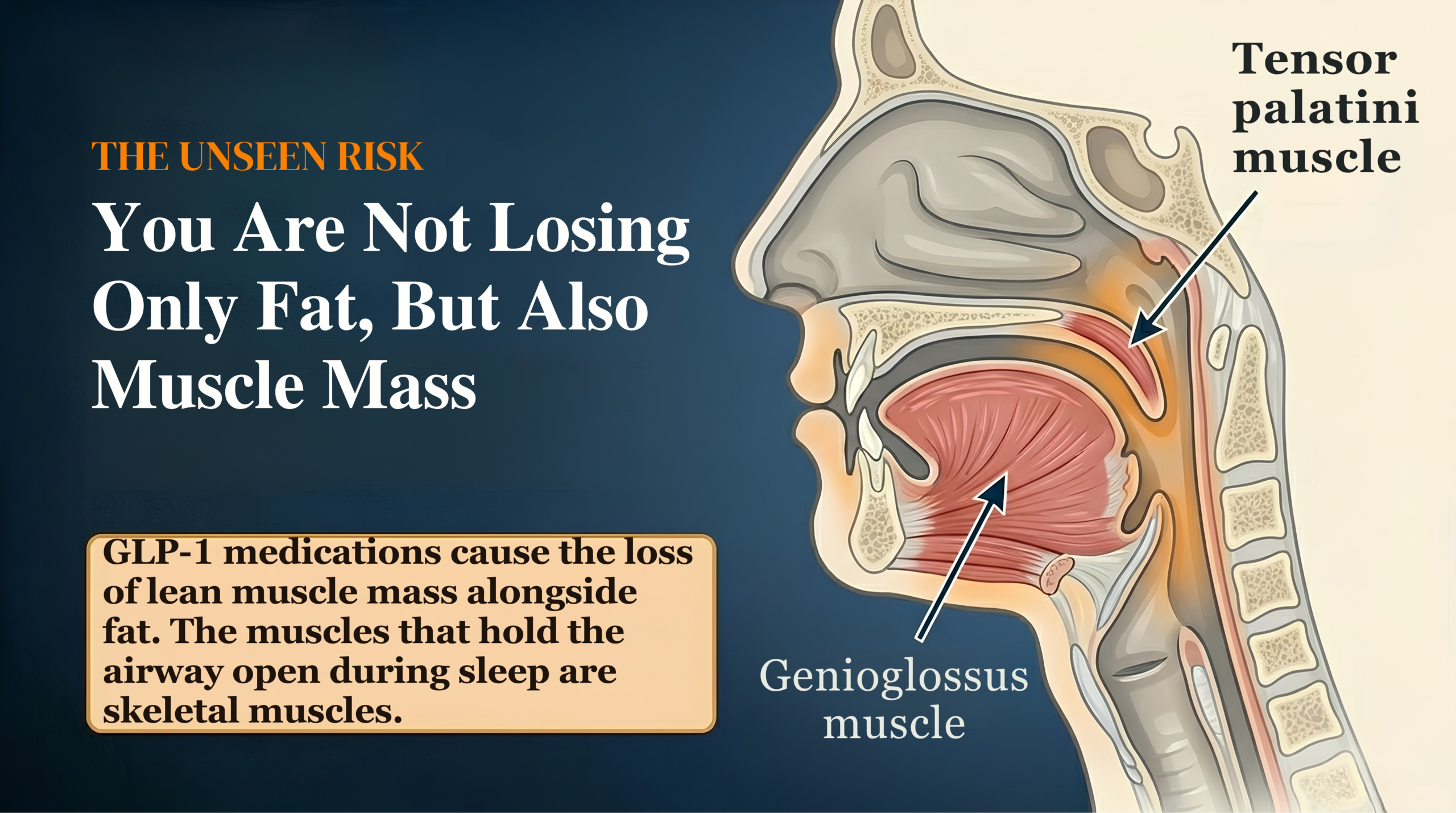
GLP-1 medications cause loss of lean muscle mass alongside fat. This is a well-documented side effect of rapid weight loss from any cause, and these drugs are no exception.
Here is why that matters specifically for sleep apnea: the muscles that hold your airway open during sleep (the genioglossus, the tensor palatini, and others) are skeletal muscles. If you lose significant muscle mass in the upper airway while losing fat around it, some of the benefit may be partially offset.
We do not yet have definitive evidence on the net effect. A dedicated clinical trial is currently enrolling to study exactly this question. But the issue is real enough to have attracted serious research attention, and it is something every patient starting a GLP-1 medication for sleep apnea should discuss with their doctor.
The practical takeaway: resistance training and adequate protein intake are not optional extras for people on these drugs. They are part of the treatment.
This Is Not a Replacement for CPAP
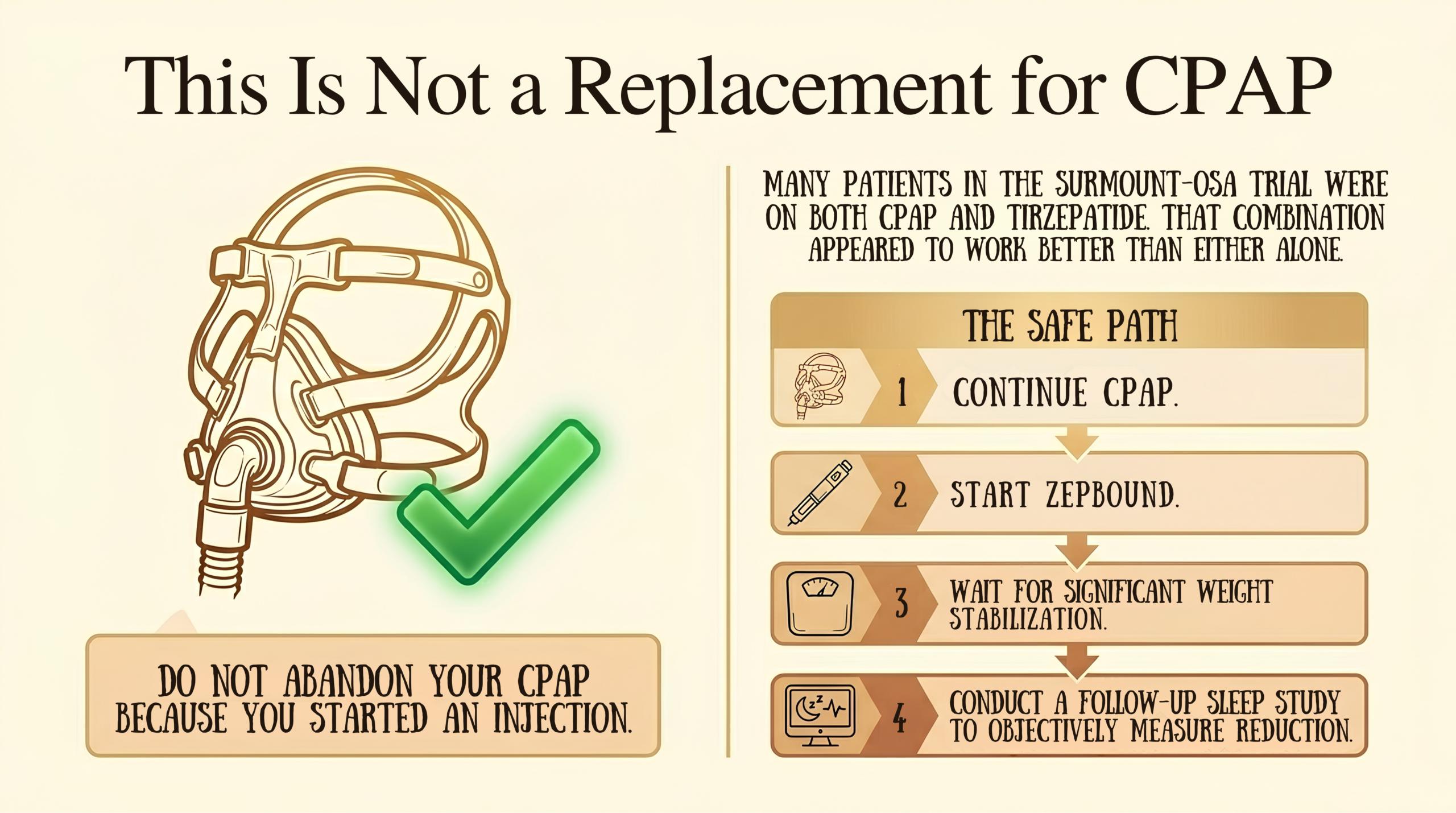
I want to be clear on this, because I suspect some patients are already using this news to justify abandoning their CPAP machines.
CPAP remains the most effective treatment for obstructive sleep apnea when used consistently. It works the night you wear it. It reduces apnea to near-zero. It has decades of evidence supporting its ability to reduce cardiovascular risk, improve cognitive function, and protect long-term health.
Zepbound works differently. It reduces the underlying anatomical problem gradually over months, and only to the extent that weight is the driver. Many patients in the SURMOUNT-OSA trial were on both CPAP and tirzepatide, and that combination appeared to work better than either alone.
If you are currently on CPAP and considering adding Zepbound, talk to your sleep specialist first. Do not stop CPAP because you have started the injection. A follow-up sleep study, not how you feel, is the right way to determine whether your apnea has resolved enough to reduce or discontinue mechanical support.
For patients who genuinely cannot tolerate CPAP, this drug may represent the most meaningful news in your treatment options in a long time. That is a real and important benefit. But the expectation should be reduction, not resolution, unless a sleep study confirms otherwise.
Who Can Actually Prescribe This and How to Navigate It
This is where patients are running into confusion, so it needs clarification.
Zepbound is not typically prescribed by your ENT doctor. Not because ENTs cannot, but because the drug requires a level of metabolic management that goes beyond the scope of a standard ENT consultation. Before prescribing, a clinician needs to screen for thyroid cancer history, pancreatic disease, kidney function, cardiovascular status, diabetes, and then manage dose titration over five months, monitor for muscle loss, coordinate nutritional support, and navigate the drug’s interaction with any planned surgery.

The right model is a team. Your ENT identifies you as a candidate, confirms the severity and type of your sleep apnea, flags obesity as the primary driver, and recognizes that you might benefit. You are then referred to an obesity medicine specialist, endocrinologist, or a GP with relevant training, who takes on the prescribing and metabolic management. Your ENT doctor remains the coordinator for the airway side: the follow-up sleep study, the surgical decisions if still needed, and the anesthetic planning if a procedure is on the table.
In practice, many patients are already finding their way to GLP-1 medications through other pathways, such as primary care, weight loss clinics, diabetes management, and arriving at ENT consultations already on semaglutide or tirzepatide. That is fine. The important thing is that the sleep apnea is monitored with objective testing, not just subjective symptom improvement.
If you want to explore whether you are a candidate, the right starting point is your sleep specialist or GP, with a clear conversation about your BMI, your OSA severity, and your goals. Come prepared with your most recent sleep study results if you have them.
A note on cost: Insurance coverage is inconsistent and, in some markets, actively in flux. List price in the US is around $14,000 per year. Some plans cover Zepbound specifically for the OSA indication, which is worth arguing for in an appeal, since the FDA label gives you ground to stand on. Others have removed it from formularies entirely. This is a conversation worth having before you start, not after.
The Bottom Line
I have followed the development of this treatment carefully, and I think the approval is genuinely worth celebrating, with clear eyes.
For patients with obesity-driven sleep apnea who cannot tolerate CPAP or who want meaningful metabolic benefit alongside airway management, tirzepatide offers something that did not exist before. Real, documented reduction in apnea severity. Real improvement in blood pressure, inflammation, and cardiovascular risk. A new option in a field that needed one.
But it requires lifelong commitment to be effective. It does not eliminate apnea the way CPAP does. It works through weight loss, so if weight is not your driver, it is not your answer. And it needs a team around it, not just a prescription.
If you are thinking about asking your doctor about it, that’s exactly the right move. Go in informed, bring your sleep study results, and expect the conversation to involve more than one clinician. The best outcomes from this drug will come from patients who understand what they are signing up for and from care teams who treat it as one tool in a broader plan, not a magic bullet.
One more reason not to delay treatment: sleep apnea does more damage than most patients realize, and not just to your heart. If you have been living with untreated or undertreated OSA, your ears may already be paying a price. The same cycles of overnight oxygen deprivation that Zepbound targets are also quietly harming your inner ear over time. I’ve written about this in detail in a separate post — Can Sleep Apnea Damage Your Hearing? — and it’s worth reading alongside this one. The case for treating OSA effectively, whether through CPAP, Zepbound, or both, is stronger than the headlines usually let on.
Free Download
Is Your Sleep Apnea Obesity-Driven?
A one-page clinical checklist to help you understand what’s driving your sleep apnea — and what to ask your doctor before your next appointment. Written by an ENT specialist. Free when you join the ENT for Everyone community.
No spam. Unsubscribe any time.
This post reflects general clinical information and is not a substitute for advice from your own doctor. Sleep apnea management should be guided by a qualified sleep specialist who knows your full medical history. If you are concerned about your sleep or breathing at night, please seek assessment from a qualified clinician.





