
Free Download
Sleep Apnea & Your Ears: The Risk Checklist
Know the warning signs. Know exactly what to ask your doctor. A one-page clinical guide written by an ENT specialist, free when you join the ENT for Everyone community.
Most people who are diagnosed with sleep apnea receive roughly the same advice: watch your weight, consider CPAP, worry about your heart. Almost nobody mentions the ears.
That is a gap worth closing.
A growing body of research now links obstructive sleep apnea (OSA) to two distinct and persistently underappreciated auditory problems: progressive hearing loss and tinnitus. Both are significantly more common in people with OSA than in the general population. Both can develop slowly enough that the connection is never made. And for hearing loss in particular, the damage may already be irreversible by the time it becomes obvious.
Understanding this link is not merely academically interesting. It changes what you do, and when you do it.
What Happens Inside Your Ear While You Sleep
In obstructive sleep apnea, the airway partially or fully collapses during sleep. Breathing stops, sometimes hundreds of times a night, and each time it does, blood oxygen levels fall. Your brain detects the problem, forces a brief arousal to restart breathing, and the cycle begins again. You may not remember any of it in the morning.
But your inner ear keeps a record.
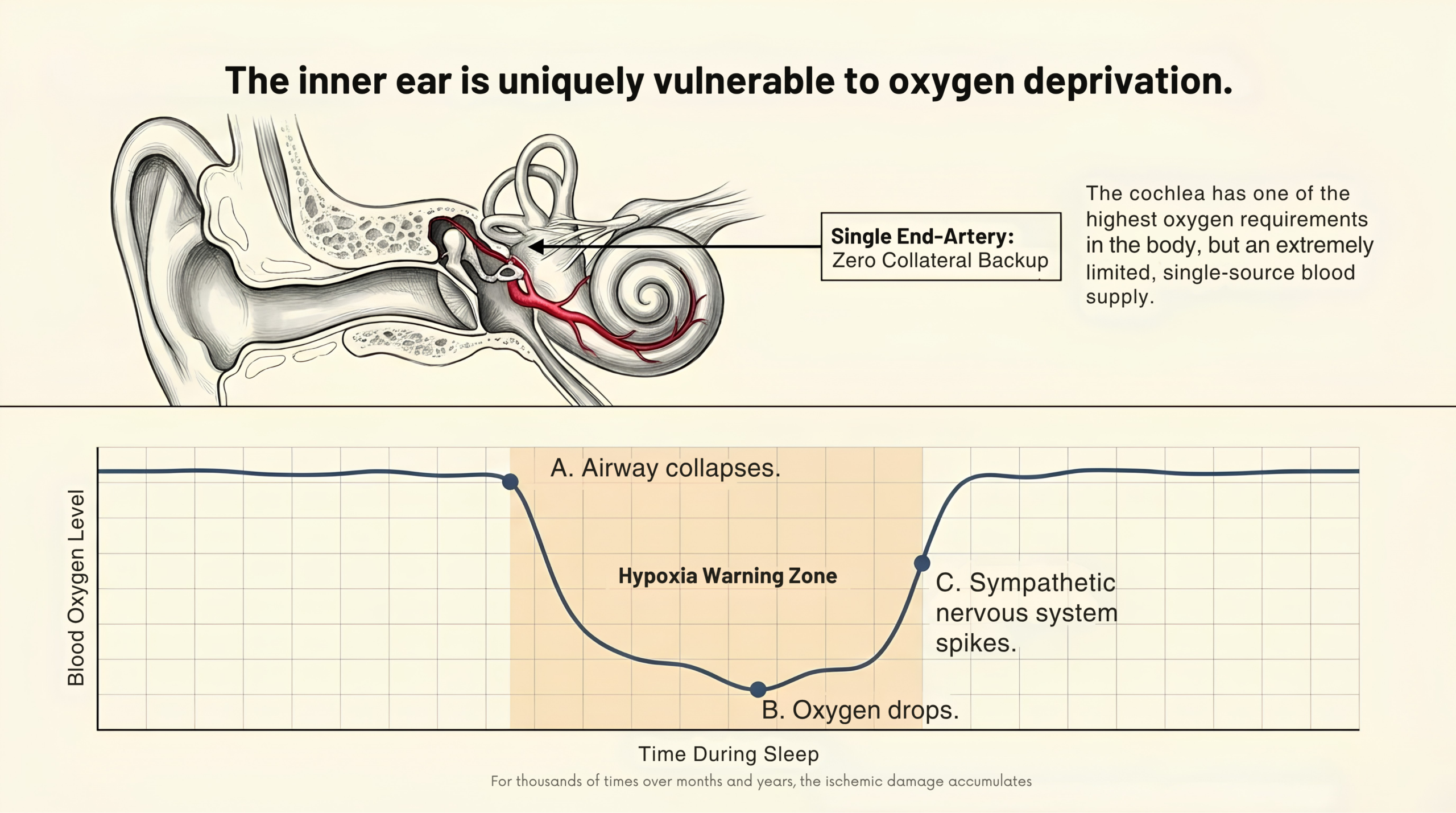
The Cochlea — Why It Is So Vulnerable
The cochlea is a tiny, snail-shaped structure deep in the inner ear responsible for converting sound into nerve signals. It has one of the highest oxygen demands in the entire body and one of the most restricted blood supplies. It relies on a single end-artery with no collateral backup. Every time your oxygen drops during an apnea event, that blood supply is compromised. Repeat this cycle thousands of times over months and years, and the damage accumulates in ways that are very difficult to undo.
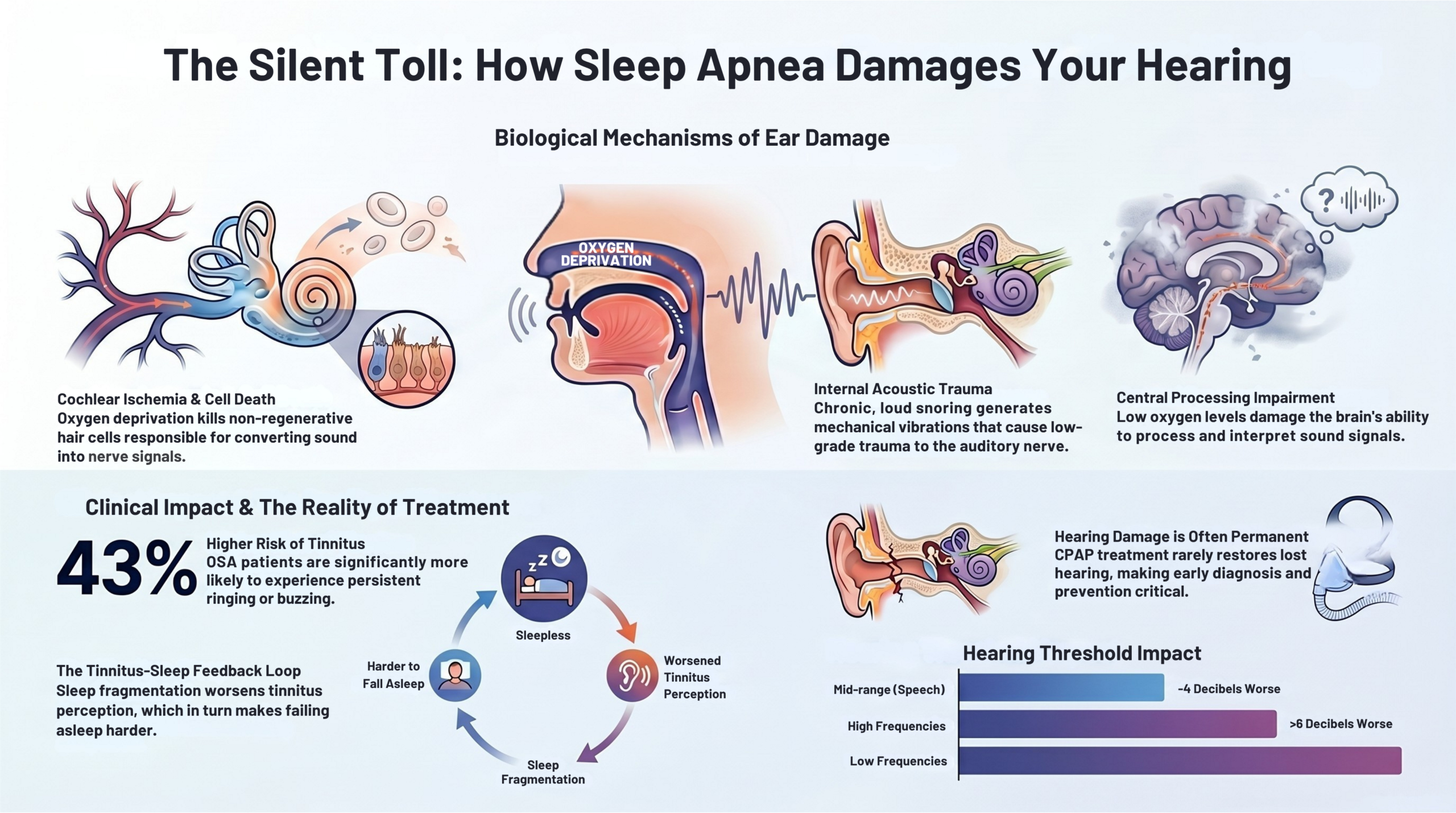
Five Ways Sleep Apnea Damages Your Hearing
Researchers have identified at least five distinct mechanisms through which OSA progressively harms auditory function. This is not a single event; it is a sustained, multi-front attack on one of the most delicate structures in the human body.
The 5 Mechanisms
Cochlear ischaemia
Oxygen deprivation reduces blood flow to the inner ear. Auditory hair cells, which handle the conversion of sound vibration into nerve signals, begin to die. Unlike almost every other cell type in the body, cochlear hair cells cannot regenerate once lost.
Oxidative stress and inflammation
Repeated cycles of low oxygen followed by reoxygenation generate inflammatory mediators that progressively damage the fine blood vessels supplying the cochlea, a process similar to ischaemia-reperfusion injury seen elsewhere in the body.
Sympathetic vasoconstriction
Each time the brain forces an arousal to restart breathing, a surge of sympathetic nervous system activity follows. Blood vessels throughout the body, including those supplying the inner ear, constrict acutely, and this happens repeatedly every night of untreated OSA.
Snoring as chronic noise exposure
Loud, chronic snoring can generate sound pressure levels at the snorer’s own ear comparable to low-level occupational noise, in some cases exceeding 40 dB continuously across the night. Over the years, this constitutes a form of self-generated noise-induced hearing loss, acting on the same hair cells already compromised by ischaemia.
Central auditory processing impairment
Chronic hypoxia not only damages the ear but also impairs the brain’s ability to process sound. Research has found that hypoxic burden (the percentage of time spent with oxygen below 90%) predicts central auditory dysfunction better than the standard AHI severity score alone.
The Hearing Loss Evidence
The research linking OSA and hearing loss is now substantial, consistent across different study designs, and difficult to dismiss.
A landmark 8-year longitudinal study using the National Health and Aging Trends Study (NHATS) dataset found that OSA is independently associated with functional hearing loss over time, acting through both cochlear damage and impaired central auditory processing.[5]
A 2023 systematic review and meta-analysis published in Otolaryngology — Head and Neck Surgery, pooling 20 studies and more than 34,000 patients, found that people with OSA had measurably worse hearing thresholds at every frequency tested, with the differences large enough to affect real-world hearing function.[1]
Key Research Findings
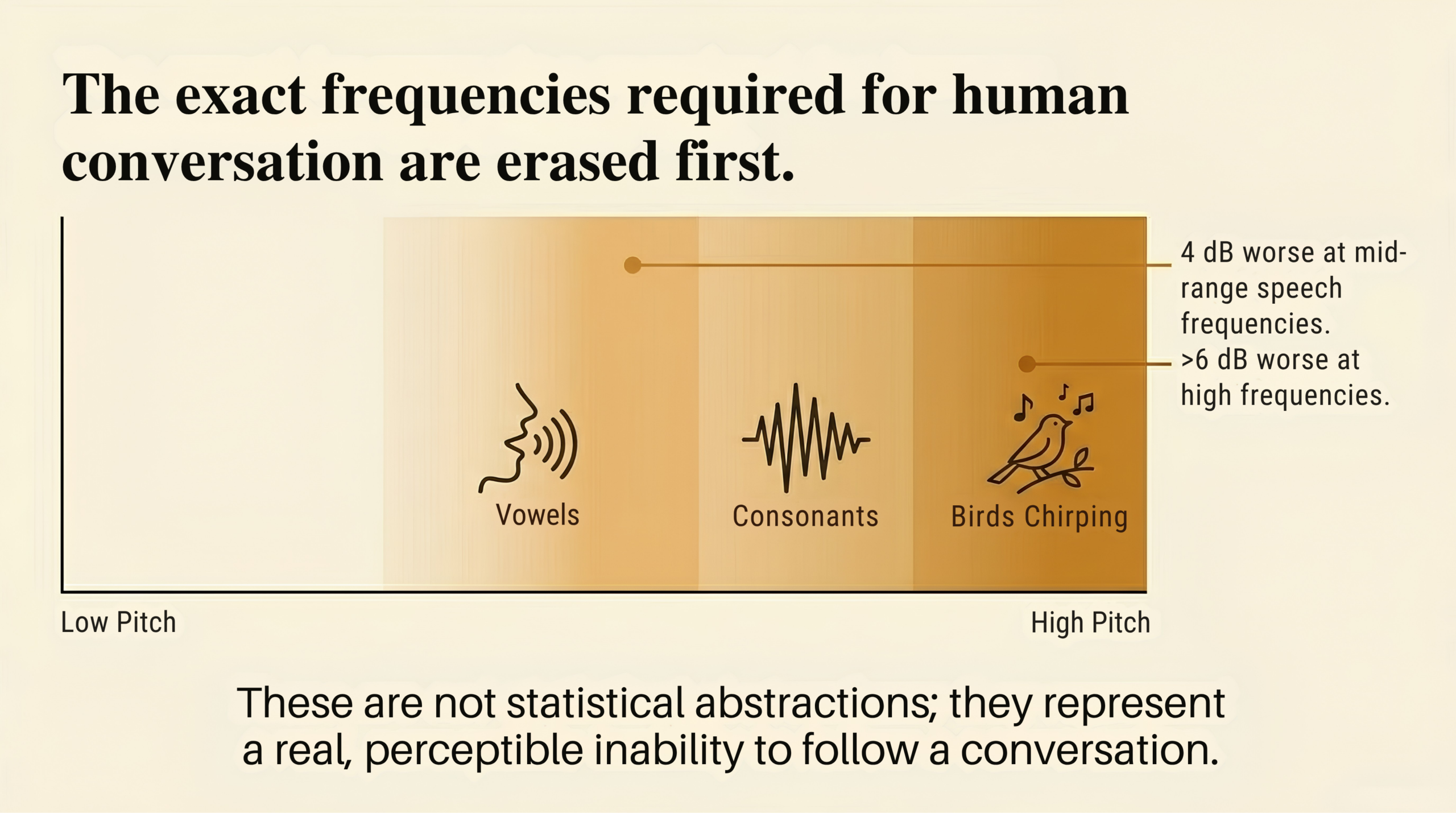
~4 dB
Worse hearing thresholds at mid-range speech frequencies in people with OSA
>6 dB
Worse at high frequencies, a perceptible difference in everyday conversation
2×
Higher risk of low-frequency hearing loss vs controls (Hispanic Community Health Study)
30%
Higher odds of any hearing impairment overall in people with OSA (Hispanic Community Health Study, 13,967 participants)
To put those numbers in perspective: a 4–6 dB difference is not a statistical abstraction. It is the difference between following a quiet conversation clearly and having to ask people to repeat themselves. In a noisy restaurant, a busy school pickup, or an open-plan office, that gap becomes significantly more apparent.
A Korean national health insurance cohort study also found that OSA significantly increases the risk of Ménière’s disease, particularly in female and middle-aged patients, who showed approximately twice the incidence compared to controls.[2]
The Tinnitus Link: A Second Injury, Often Overlooked
Hearing loss is not the only auditory consequence of sleep apnea. Tinnitus — the ringing, roaring, or buzzing in the ears that has no external source – is separately and significantly elevated in people with OSA, and it tells a somewhat different story.
A 2025 study published in Sleep and Breathing, using NHANES data from 4,871 US adults, found that people with OSA were 43% more likely to report tinnitus compared to those without it (OR = 1.43; 95% CI 1.05–1.94), after adjusting for all relevant confounders.[3]
Several of the same mechanisms responsible for cochlear hair cell damage also generate tinnitus. When the cochlea is under stress or structurally compromised, it sends disordered signals up the auditory nerve. The brain, attempting to compensate for reduced input, turns up its own internal sensitivity, a process called central sensitisation, which produces the phantom sound you experience as tinnitus.
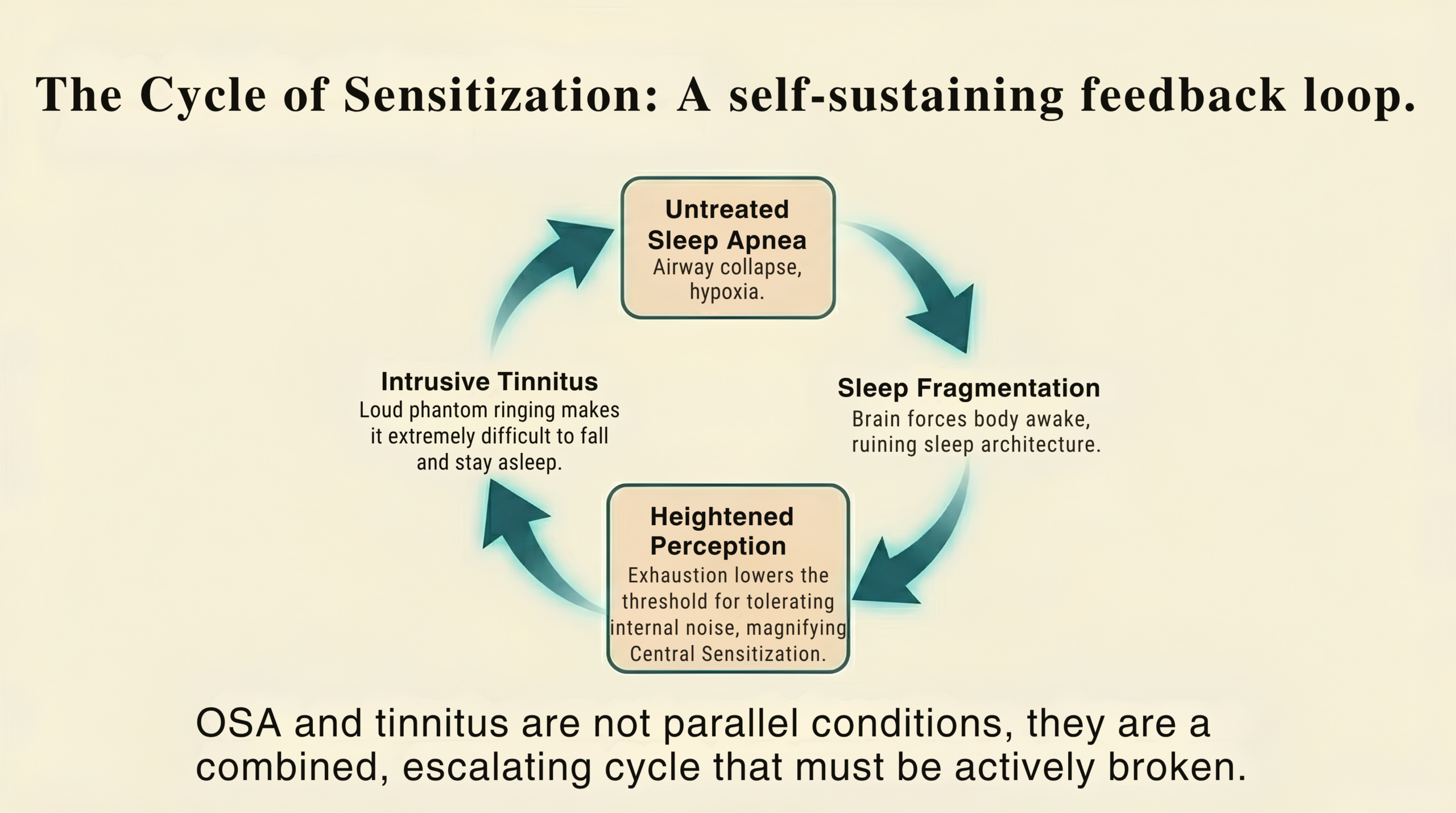
Poor sleep amplifies all of this. Chronic sleep fragmentation lowers the threshold at which the auditory system perceives internal noise, making tinnitus louder and more intrusive even when the underlying cochlear damage is modest.
The Feedback Loop
Sleep apnea fragments sleep → heightened tinnitus perception → intrusive tinnitus disrupts sleep further → deeper sleep fragmentation → worsened tinnitus.
Both conditions sustain and amplify each other. This cycle can be genuinely difficult to interrupt once it is established, which is one of the strongest arguments for treating sleep apnea before it takes hold.
Free Resource
Already have tinnitus?
Use the free ENT for Everyone Tinnitus Tracker to log your symptoms, identify patterns over time, and generate a clinical summary you can share with your ENT specialist.
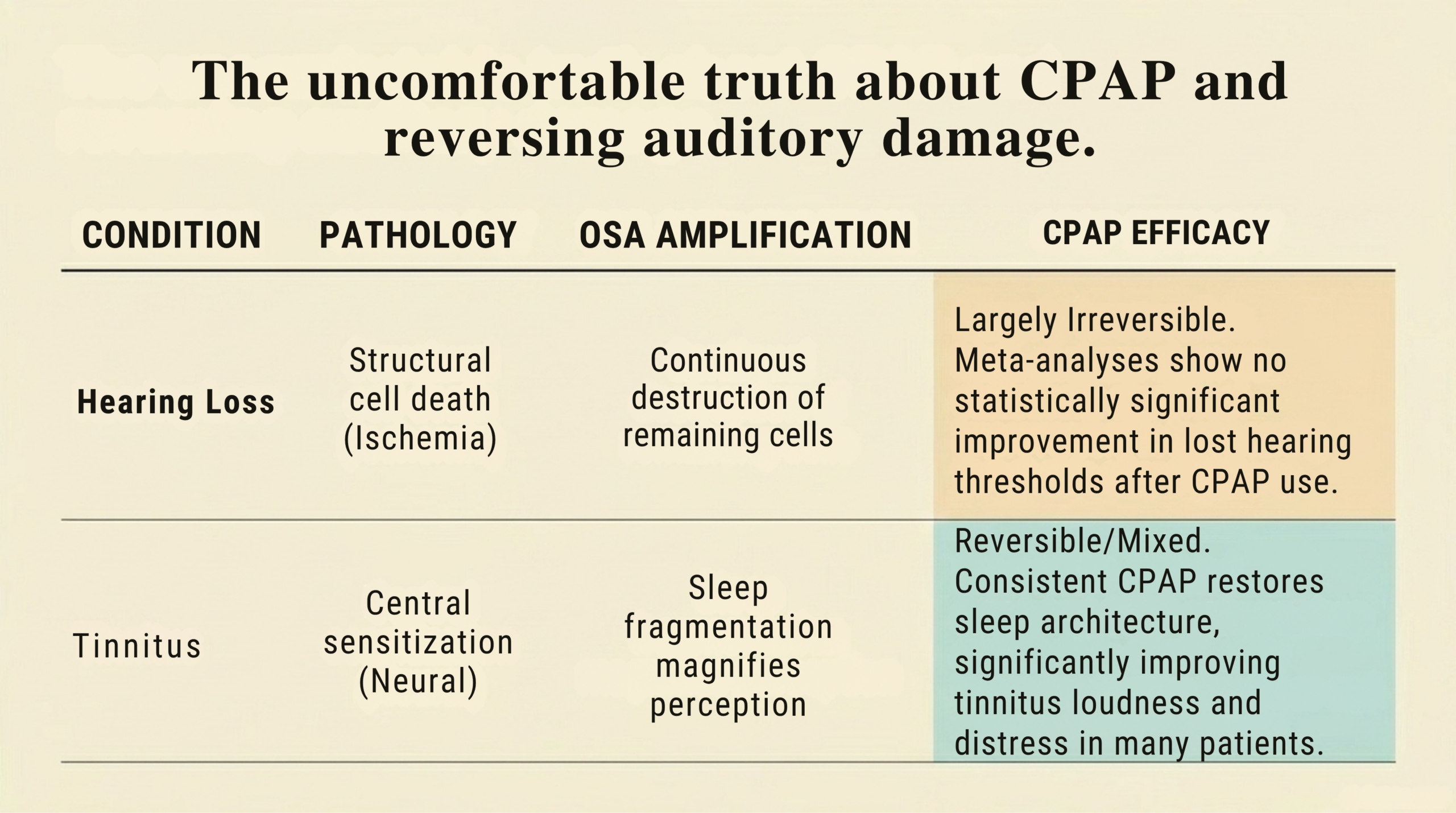
The Uncomfortable Truth About Treatment
This is where the evidence becomes harder to hear and where the case for acting early becomes most compelling.
Common Misconception
“Starting CPAP will fix my hearing damage.”
This is not what the evidence shows. Treating sleep apnea is important and worthwhile, but it does not reliably restore hearing that has already been lost. Prevention, not reversal, is the goal.
For hearing loss, the 2023 meta-analysis found no statistically significant improvement in mid-frequency hearing thresholds following CPAP treatment across the pooled studies.[1] The ischaemic damage to cochlear hair cells, accumulated over years of untreated OSA, appears to be largely irreversible. One smaller study did find modest improvements at low and mid-frequencies after six months of CPAP use, suggesting there may be a therapeutic window early in the disease course, but this finding represents the exception in the literature, not the rule.
For tinnitus, the picture is slightly more encouraging. Because part of the tinnitus burden in OSA is driven by central sensitisation and sleep fragmentation rather than permanent structural cochlear damage, some patients do experience genuine improvement in tinnitus loudness and distress once CPAP restores normal sleep architecture and stabilises overnight oxygen levels. The evidence is mixed, not every patient improves, but it is more promising than for hearing loss alone.
It is also worth noting that CPAP is not the only treatment for OSA. For patients who cannot tolerate it or whose anatomy suits other approaches, alternatives include mandibular advancement devices (custom-fitted oral appliances that keep the airway open), positional therapy (for position-dependent apnea), weight management, and in selected cases, surgical options such as septoplasty, tonsillectomy, or upper airway procedures. The right approach depends on the individual; a sleep specialist or ENT can advise on which is most appropriate.
The practical conclusion is the same in both cases: the best time to act is before the damage accumulates. Treating sleep apnea early, before cochlear injury is established and before the tinnitus-sleep cycle takes hold, is the only reliable way to protect your hearing.
What to Do: A Practical Guide
If any of the following situations apply to you, it is worth taking action now rather than waiting to see how things develop.
| Your Situation | Recommended Action |
|---|---|
| You snore loudly, wake feeling unrefreshed, or have been told you stop breathing in your sleep | Ask your GP about a sleep study. Home-based testing has made this considerably more accessible than it once was. |
| You have diagnosed OSA and have noticed changes in your hearing — turning the TV up, missing words, struggling in background noise | Mention this at your next appointment and ask for a comprehensive audiological evaluation. Request high-frequency testing and speech-in-noise assessment, not just a standard tone audiogram. The standard test alone can miss early OSA-related changes. |
| You have OSA and experience ringing, buzzing, or hissing in your ears, particularly at night or when trying to sleep | Tell your ENT specialist. The two problems are often related, and knowing that changes the clinical approach. |
| 🔴 Sudden loss of hearing in one or both ears | Seek same-day ENT review. Sudden sensorineural hearing loss is a medical emergency. Treatment is time-sensitive; delays reduce the chance of recovery. |
| 🔴 Tinnitus that pulses or beats in time with your heartbeat | This requires ENT investigation to rule out a vascular cause. Do not wait for a routine appointment. |
If you have been putting off addressing your sleep apnea because it feels manageable, your ears are one more reason not to wait. The effects of untreated OSA on hearing are slow, cumulative, and largely silent.
Sleep is not passive. It is the body’s most demanding maintenance shift, the hours during which the brain consolidates, the immune system repairs, and the vascular system restores.
We tend to think of disrupted sleep as something we catch up on. What the cochlea loses during years of nightly oxygen deprivation is considerably harder to recover.
Frequently Asked Questions
Can sleep apnea cause permanent hearing loss?
Yes. The cochlear hair cell damage caused by repeated oxygen deprivation during apnea events is largely irreversible. Current evidence suggests that starting CPAP does not restore hearing that has already been lost, which is why early diagnosis and early treatment are so important.
Will CPAP improve my tinnitus?
Possibly, for some patients. Because part of the tinnitus burden in OSA is driven by sleep fragmentation and central sensitisation rather than permanent cochlear damage, some people do notice genuine improvement once CPAP restores normal sleep architecture and oxygen levels. The evidence is mixed, not all patients experience this, but it is more encouraging than the evidence for reversing hearing loss.
How do I know whether my hearing loss is connected to my sleep apnea?
There is no single test that establishes OSA as the definitive cause of a given person’s hearing loss, it is a diagnosis of association. An ENT specialist will take a full history, arrange comprehensive audiological testing, and consider OSA as a contributing factor alongside other causes such as noise exposure, age-related change, and genetic factors.
What type of hearing test should I ask for?
Ask for a comprehensive evaluation that includes high-frequency pure-tone testing (beyond the standard 4 kHz ceiling) and a speech-in-noise assessment. OSA-related changes can affect high-frequency thresholds and central processing, both of which may be missed on a basic tone audiogram alone.
My snoring is not that loud. Do I still need a sleep study?
Snoring volume is not a reliable indicator of OSA severity. Some people with significant apnea snore quietly; others snore loudly with minimal airway obstruction. More reliable indicators include waking unrefreshed despite adequate sleep time, persistent daytime sleepiness, and a partner observing breathing pauses. If any of these apply, speak to your GP about a sleep study, home-based testing is now widely available.
References (Vancouver format)
- Kasemsuk N, Chayopasakul V, Banhiran W, Prakairungthong S, Rungmanee S, Suvarnsit K, et al. Obstructive sleep apnea and sensorineural hearing loss: a systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2023;169(2):201–209. doi: 10.1177/01945998221120777. PMID: 36040818
- Kim JY, Ko I, Cho BJ, Kim DK. Association of obstructive sleep apnea with the risk of Ménière’s disease and sudden sensorineural hearing loss: a study using data from the Korean National Health Insurance Service. J Clin Sleep Med. 2019;15(9):1293–1301. doi: 10.5664/jcsm.7922. PMID: 31538600
- Wang C, Shi M, Xie L, et al. Association between obstructive sleep apnea and tinnitus in the United States: NHANES 2005–2020. Sleep Breath. 2025;29:86. doi: 10.1007/s11325-025-03243-0
- Chopra A, Jung M, Kaplan RC, Appel DW, Dinces EA, Dhar S, et al. Sleep apnea is associated with hearing impairment: the Hispanic Community Health Study/Study of Latinos. J Clin Sleep Med. 2016;12(5):719–726. doi: 10.5664/jcsm.5804. PMID: 26951413
- Jiang K, Spira AP, Reed NS, Lin FR, Deal JA. Obstructive sleep apnea and functional hearing loss over 8 years: results from the National Health and Aging Trends Study. Am J Epidemiol. 2026 Jan 13:kwag006. doi: 10.1093/aje/kwag006. PMID: 41526194
Medical Disclaimer
This article is for educational purposes only and does not constitute medical advice. The information provided is intended to help patients understand a medical condition, it is not a substitute for a consultation with a qualified healthcare professional. If you have concerns about your hearing, tinnitus, sleep, or any of the symptoms described in this article, please speak with your GP or an ENT specialist. Do not delay seeking medical advice because of something you have read online.
Dr. Carmen Chiran MD, PhD — ENT Specialist & Surgeon
Approximately 20 years of clinical experience across the UK, Ireland, and UAE. Founder of ENT for Everyone — a patient education platform built on the conviction that an informed patient is healthier. entforeveryone.com





